It would be nice if human hospitals could give the LLLT attention Ron gives his animal patients.
For more on THOR pet treatments click here
For more on LLLT training click here
 Featured Testimonials
Featured TestimonialsIt would be nice if human hospitals could give the LLLT attention Ron gives his animal patients.
For more on THOR pet treatments click here
For more on LLLT training click here
Does LLLT make you thinner? a Harvard research group investigates, LEDs for muscle function in patients with chronic obstructive pulmonary disease and laser vs needles for myofascial trigger points. There is my own introductory paper on LLLT for dentists, another review of laser and LED treatments for neurological and psychological applications, a TMJ study, and a trial of class IV laser for epicondylitis (see my rant “LLLT companies may be no better than Big Pharma“).
Continue reading
It is a popular sport in the LLLT industry to sneer at Big Pharma for their side effects and marketing practices, but the LLLT industry is far from criticism itself. Whilst LLLT side effects are hard to find, marketing overstatement and misdirection are common place.
In this months literature watch is a paper titled “The Effectiveness of Therapeutic Class IV (10 W) Laser Treatment for Epicondylitis”. This small study showed that 10 Watt Class IV laser (mixed 8W 970nm, 2W 810) was successful in reducing pain and improving function in an RCT with 15 patients, and that there was good statistical significance at 6 months following a course of 6 treatments.
The claim by class IV laser manufacturers is that class IV lasers are better (faster, deeper and more effective) than Class 3b and LED systems. Conversely the 3B laser and LED manufacturers argue that less power density is more effective because delivering energy too quickly can overdose tissues and class IV lasers might burn the skin.
Throughout this paper there are marketing messages claiming the advantages of shorter treatment times than low power LLLT systems and of course the title shouts “10 Watt Class IV laser” just in case the reader is in any doubt that more power is what you need.
Regular readers of this column know my obsession with irradiation parameters, particularly dose rate effects (W/cm2) and will not be surprised to learn that I deconstruced the irradiation parameters used in this trial . Surprise, surprise they were the same low irradiance levels typically used by 3B lasers and LED systems, if not less and the treatment time was longer too.
Yes, it was a 10 Watt laser and yes, 3,000 joules was delivered, however it had a very large beam area and treatment was delivered over a very large area (45cm2) in a “painting fashion”. The fluence (dose) was 6.6 Joules/cm2 and the power density was a tiny 22mW/cm2, consequently treatment time was a hefty 5 mins.
The average irradiance was not disclosed in the paper and the reader is directed to think that more power is quicker. Perhaps LLLT companies are no better than the pharma industry when it comes to disseminating specious information.
P.S. research trials with 3B lasers are typically 30 seconds to 3 mins and our recommended treatment is 1 min with a large LED cluster to the lateral epicondyle and 30 seconds for any related trigger points.
Attend a THORLaser One Day Training Course to see the research and get all the information in making an informed decision: https://www.thorlaser.com/courses/
25 new LLLT papers for you this month including clinical trials on Bells palsy, orthodontic pain, herpes zoster ophthalmicus and orthognathic surgery. There are reviews on dentine hypersensitivity, muscle contractile function, postexercise recovery and infarct volume after stroke. Some interesting laboratory studies on bone marrow in mice, early vs delayed LLLT application on nerve regeneration, bone remodeling during induced tooth movement in rats and LED vs ultrasound for tendinitis.
Continue reading
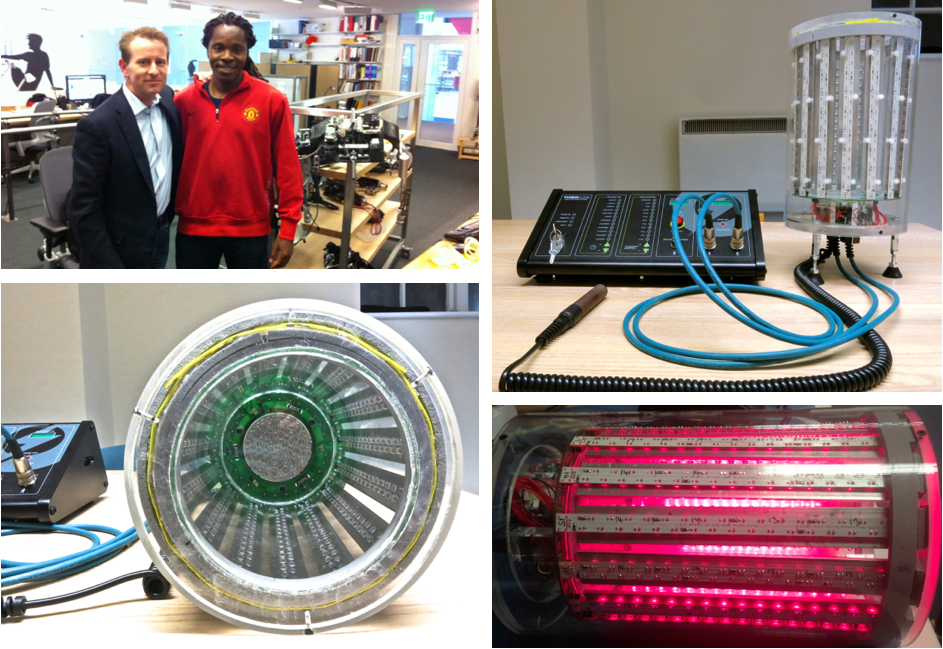
David Sengeh has been developing powered limbs at MIT for amputees (like the bionic man). Where the powered limb attaches to the body (the stump of the original leg) it gets very sore. David has been using our standard THOR products to heal the stump and reduce pain. It works very well, though it takes a lot of time to treat the whole area. I am in Boston now to help David start clinical trials with a new device we designed that will treat the whole stump. The amputee puts the the leg stump into the LED treatment cylinder and gets a complete treatment in just one minute :-)
In the BMJ Last Saturday Anita Jain wrote “Gold jewellery, cars or an exotic foreign holiday, these are among the luxury gifts listed in a parliamentary committee report as being used by pharmaceutical companies to coax doctors into prescribing their drugs”. She goes on to describe the “3C strategy” employed by drug companies. “convince if possible, confuse if necessary, and corrupt if nothing else works”. Many (she says) will say an emphatic no to luxury gifts, but what about discounts, conference fees, hotels and flights?
Since we have been working with more doctors these days (rather than therapists) I am being approached with requests for hotel and flight costs and I confess I have conceded.
Why does this happen?
a) Because this is the world they live in (i.e. it is normal to have industry pay)
b) Academic and educational budgets are tight and industry has more money than it knows what to do with (they think).
So what should I do ?
I have conceded and paid out a few times, but not with any enthusiasm as we are not yet making $ billions in profits, but my conscience wrestles with it. I do not want to be guilty of behaving like bad pharma but then again I want our product to be accepted by mainstream medicine, so what should I do?
Comment below
33 new LLLT papers for you this month including: a review of 21 papers on muscle performance, fatigue and repair, a controlled multicenter trial on male pattern baldness, another trial on oral mucositis and how about this, 810nm laser ameliorates diabetes!
Continue reading